
Patellofemoral stabilisation
Many patients experience one episode of dislocation of the patella with no further recurrence. In this instance surgery is not required. There are some patients whose patella dislocates only occasionally with minimal incapacity. These can be treated with leg strengthening exercises or braces.
For patients who experience recurrent patella dislocation, patellofemoral stabalisation surgery is indicated.
Procedures for Patellofemoral stabilisation
There are a number of surgical options available and the options chosen will be based on the biomechanical abnormalities causing the patella to dislocate. These surgeries include:
Medial Patellofemoral Ligament Reconstruction
In the last twenty years this has become the mainstay for treatment of patella instability. The medial patellofemoral ligament is almost always stretched or torn when the patella dislocates laterally (in an outward direction). A reconstruction of this torn ligament provides more reliable results than a simple repair or tightening of this ligament. The semitendinosus tendon (inside hamstring) is the most frequently used graft of choice to perform this reconstruction. It is often combined with a release of the lateral retinaculum if that is abnormally tight. See Figure 1.
Tibial Tubercle Transfer
This is indicated when the insertion of the patella ligament is abnormally located on the outer part of the tibia. The procedure involves cutting a small sliver of bone at the tibial attachment of the patella ligament and shifting it medially (inward). It is usually held with two screws.
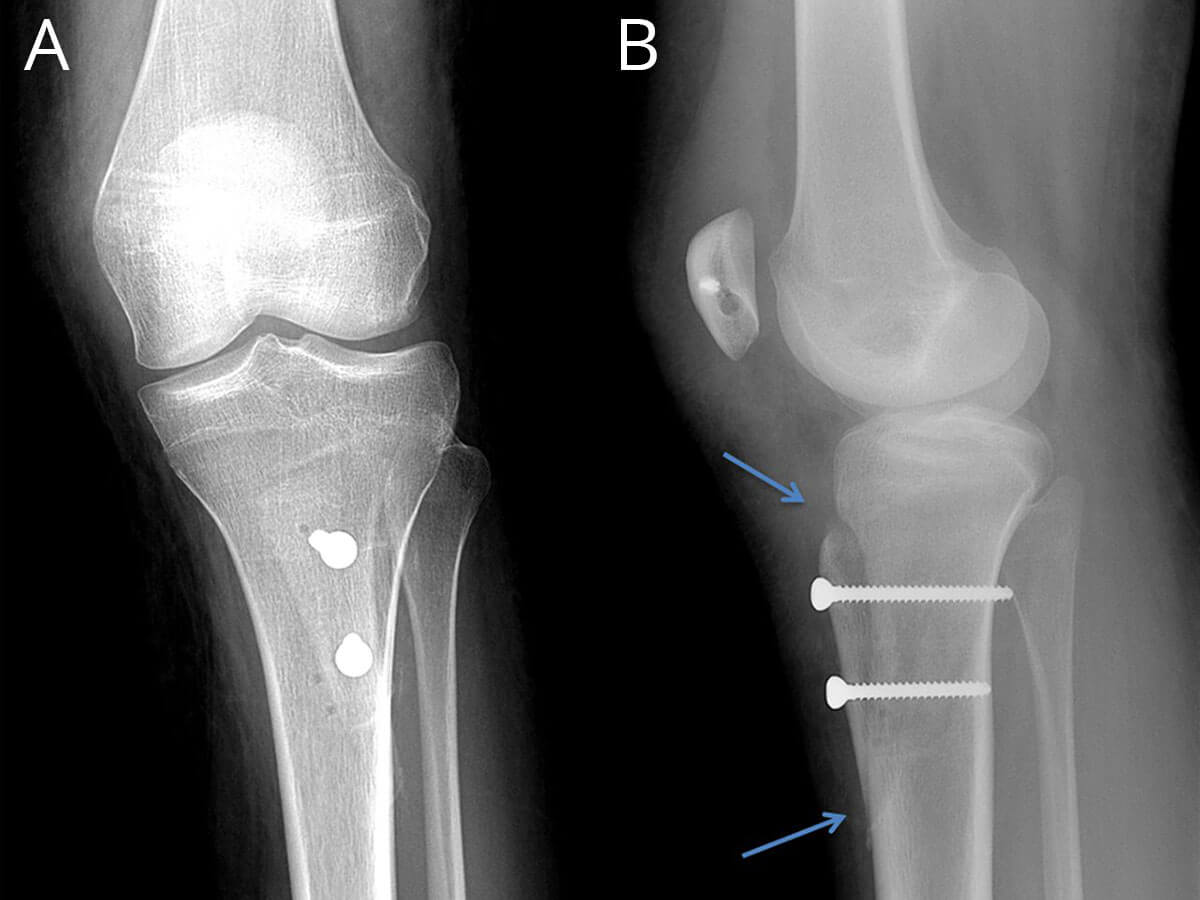
Fig 3: Tibial tubercle osteotomy.
Trochleoplasty
This procedure is rarely performed but is indicated when the trochlea is excessively shallow or flat. This is a technically challenging procedure but can lead to very satisfactory results in the most challenging cases of patella instability. The aim of this technique is deepen the femoral trochlea in order to hold the patella in place.
Distal Femoral Osteotomy
Some patients with patella instability have excessive inward twist of their lower femur (femoral anteversion). If this is a significant cause of the instability it will need to be treated with a distal femoral osteotomy. This procedure involves breaking the lower part of the femur and rotating it outwards.
Two or three of the above surgical options may need to be performed together where indicated.
Preoperative investigations
All patients should have an X-ray as well as a CT scan to assess the cause of the instability.
Post operative care
For most procedures a straight knee brace will be applied in the operating theatre. This is to be worn for up to four weeks post-operatively. Most patients will go home on crutches on the day following surgery. A physiotherapist will assist the patient with the use of crutches and simple exercises to be done at home. Patients will be reviewed at two weeks to check the wound and to assess progress.
Recovery from this procedure will take several months. Physiotherapy is essential to strengthen the quadriceps (thigh muscle) as well as to assist in regaining knee movement.
Complications
- Infection
- Deep venous thrombosis
- Numbness on the outside of the wound
- Ongoing instability of the patella.
Outcome
Although it can take some time to recover from this procedure the overall results are very good in preventing further patella dislocations. However, this operation will not alleviate patella pain if that was present prior to surgery.